Ph.D. research Project
How Design Can Contribute to Children's Neurological Rehabilitation? Case study: Co-Designing Paediatric Rehabilitation Programs for Learning Disabilities.
Research Supervisor: Prof. Rocco Antonucci, University of Genoa, Italy.
Thesis defended on March 30, 2015 at Università IUAV di Venezia, Italy. Obtained degree - Ph.D. in Design Science.
This project was realized in collaboration with:
- Casimiro Mondino National Neurological Institute - Foundation and University of Pavia, Italy.
prof. Umberto Balottin (Head of the Infant Neuropsychiatry Department)
Dr. Marina Zoppello (Psychologist, psychotherapist)
Dr. Luca Capone (Psychologist, psychomotricist)
- NeuroLab DIBRIS - Department of Informatics, Bioengineering, Robotics and System Engineering, University of Genoa, Italy.
Prof. Vittorio Sanguineti (Associate Professor of Biomedical Engineering)
Irene Tamagnone (Ph.D. Student)
The purpose of this research was to identify the role of designer in project development of children’s rehabilitation programs and to verify the contributes that can be brought into this area by application of proper design approaches, dedicated design research and evidence based design solutions.
Children's neurological rehabilitation was taken as an example of extremely sensitive, delicate and complex field of design where approaches to project development are supposed to be a subject of careful studies and evaluations. However, the results and findings of this research could be usefully applicable in other industrial domains as well.
While planning the work on this ph.d. project a set of classical research methods were defined, such as: literature review, observation and interviews; these were followed by a practical part - development of case study and realization of co-design project with the team of related professionals.
Literature review deals with the following arguments:
- Neurological disorders: overview, classification
- Learning Disabilities
- Models of neurological rehabilitation
- Review of existing rehabilitation programs for Learning Disorders
- Theoretical and methodological bases of Healthcare Design:
- Evidence-based design principles
- Theory of Supportive design
- Neuroesthetics
- Paediatric neurorehabilitation. Play therapy
- Designing for Children
- User Experience Design for Children
- Age-appropriate toy Design
- Co-design with children
- Co-design with doctors and researchers
- Factors that influence product development
- Technological review:
- Tangible interactive interfaces
- Rehabilitation Robotics
- Haptic feedback devices
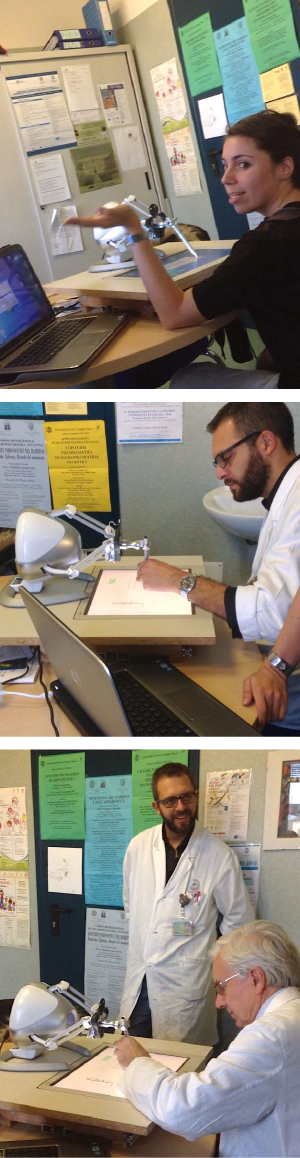
OBSERVATION AND INTERVIEWS IN FIELD WITH DOCTORS AND THERAPISTS
Identifying and studying target diseases and problematic factors influencing rehabilitation process (Pict. 1)
During the consultations at Infant Neuropsychiatry Department of Mondino National Neurological Institute, two main fields of children’s neurological rehabilitation were suggested as perspective for possible design interventions.
Learning disorders and in particular reading and writing disorders (Developmental Dyslexia and Dysgraphia)
Motor disorders like limb paralysis caused by injuries or Cerebral Palsy (e.g. Hemiplegia)
Pict. 1 Summary Diagram: Doctors’ point of view on problematic factors influencing children’s rehabilitation process [click to enlarge]
CASE STUDY 1 "DYSLEXIA"
Link between Visual Spatial Attention and Reading Acquisition was hypothesized and proved experimentally by researcher Andrea Facoetti from the Developmental and Cognitive Neuroscience Lab, University of Padua. His research team demonstrates that only 12 hr of playing action video games not involving any direct phonological or orthographic training drastically improve the reading abilities of children with dyslexia.
Since our team was very enthusiastic about the results of Andrea Facoetti, we decided to work in the same direction proposing some kind of design improvement for even better efficiency. "Why not to add the third dimension?" our idea was. The rehabilitation video games may be projected in 3D, with the very high definition, providing the immersion issue, to the process of exercising.
The validity of idea was immediately confirmed by prof. Ballotin, the Head of Infant Neuropsychiatry Department, who explained that with the addition of deepness into the gaming experience can activate more nearby cerebral zones, accelerating the recovery of neural connections and consequently making the rehabilitation process more efficient.
Moreover, Dr. Capone, the psychomotricist of Infant Department noticed that actually that kind of spatial exercises in stereoscopic environment could be performed by means of motion control technologies which will be definitely useful also for the patients with motor disorders like hemiplegia and other paralysis. Rehabilitation programs for them normally require different types of physical activity, repetitive movement exercises. Thus our engaging and motivating therapeutic game will suite them well.
Thereby our rehabilitation system for Dyslexia became the Multifunctional one.
Concept of new multifunctional rehabilitation system: Tangible video game with virtual immersive age-adapted environments, for visual-spatial attention and motor training (Pict. 3)

Pict. 2 Concept graphic model of Multifunctional Rehabilitation System
The rehabilitative game takes place in a 3-dimensional interactive environment in front of the wall-screen with stereoscopic projection.
Players wear lightweight passive polarized glasses adapted for the children’s ergonomic needs to perceive an effect of stereoscopic projection.
Players interact with the game elements via motion controllers, freely moving in space of play-rehab room.
Motion controllers has and adoptive design in order to suit patients with difficulties to grab and hold controller in their hand (special clasp system, will allow to securely attach controller to the patient’s hand or arm).
Video-game may involve more than one player (game-companion may be the therapist itself, other patient, friend or parent). Additional competitive motivation for better engagement into play therapy.
Computer software suppose to collect all the results and parameters of rehab session performance into a patient’s personal progress database, in order to analyse and monitor the improvements, automatically augmenting the difficulty level of the game.
1 - Computer with rehabilitation game running on it (individual settings of difficulty and speed, according to the patient’s achievements), collecting results into personal patient’s database of progress.
2 - Polarized 3D stereoscopic projector with high resolution up to 4K
3 - Special screen for 3D polarized projection
4 - Moving 3D elements of the game to interact with
5 - Passive 3D glasses adapted for children’s use
6 - Motion controller (the instrument of interaction with the game; adaptive design, also for children with limb paralysis)
The 1st case study "Dyslexia" was paused at the phase of concept, leaving space to the 2d case study “Dysgraphia“ which was considered more promising in terms of realization and expected results, together with the higher necessity of rehabilitation program improvement at the collaborating rehab facility and lack of researches dedicated to this learning disorder.
Case study 2 “Dysgraphia“
Once the target disorder was determined, we moved to the step of consultations with therapists, in order to understand the principals of rehabilitation process.
They explained that the basic skills involved in the process of handwriting are: movement coordination, orientation and organization of space and time, the eye-hand coordination, awareness of the body scheme, sequential memory, language, the sense of rhythm (usually poor), the process of symbolization (slow), the ability to discriminate sounds-signs.
Also dysgraphia may be an associated disorder in presence of other learning disability, but not necessarily related to them.
So, the possible intervention program can be divided into two main tracks that need to be undertaken in parallel:
- Exercises aimed at the development of basic skills
- Specific writing exercises
The first track of rehabilitation program is supposed to reduce the weaknesses identified in basic skills; The second track aims to promote the recovery of writing skills appropriately.
These two tracks should be offered to the patient in parallel and gradually through play exercises that require the development and enhancement of single skills, as well as exercises-games that require the development of various skills all together, to avoid the delay in conquesting grapho-motor ability that gratifies the child, allowing him to be more self-confident, experiencing positive results also at school. Important basic skills to work on are:
- perception
- space-time organization
- integration of space and time (rhythm)
- body scheme control
- balance and coordination
- relaxation
- laterality
- visual-motor and eye-hand coordination.
As the next step of project, during our brainstorming conversation therapists suggest trying the mechanism of mirror neurons activation while practicing the described above rehabilitation interventions. The idea is that by watching and actually feeling the correct handwriting or hand-drawing movement, you learn, and can easily repeat the same on your own.

Pict. 3 Concept graphic model of Interactive Robotic Rehabilitation System for Dysgraphia
TECHNOLOGICAL SOLUTION PROPOSAL, PROTOTYPE DESCRIPTION
SYSTEM COMPONENTS AND ITS FUNCTIONS
Equipment kit (Pict. 3) consists of:
1 - Robotic arm (or haptic manipulation device like The Geomagic Touch formerly Phantom Omni, Novint Falcon or similar)
2 - Pen (stylus) attached to the endpoint of robotic arm
3 - Tablet with interactive game application running on it.
4 - Laptop, that controls the whole system with the administrator’s version of program (for doctors, therapists, or parents) running on it. Program contains database of patients' virtual folders with all the parameters of therapeutic performance.
Possibility of remote monitoring.
Functioning of hardware and software interfaces.
Physical interface (hardware)
Robotic arm or haptic device with 4 operation modes:
Learning Mode (LM)
Robotic arm of haptic device “learn” from expert-user (therapist/administrator/ developer) the correct writing movement of particular letter/word/track in order to reproduce it in therapeutic modes (GM, AM)
Guided mode (GM)
Aimed to assist learning, understanding and memorizing the correct writing movement: patient grips the pen and keeps the hand relaxed, leaving the robotically actuated pen guide him through the writing (or pre-graphic) exercise.
Gradual Autonomous mode (AM)
Aimed on practicing of previously learned movements. Patient reproduce the same graphic element by the force of own hand, with the pen gripped but not powered by robotic assistance. In case of significant motion errors the robotic correction will be applied – resistance feedback, oriented towards the correct writing track.
Moving forward in rehabilitation game, getting over the difficulty levels makes correction feedback force decrease gradually up to disappear completely, leaving the total motion freedom to the patient.
Gradual Counteractive mode (CM)
Activates in the last phase of the rehabilitation process (when the child is already familiar with the pen and has recovered most of the writing skills). It is a sort of physical exercise to strengthen the muscles of patient’s hand.
Robotically actuated pen pushes out from the correct path, creating obstacles for writing, the patient have to apply more force to stay within the specified ranges and be able to complete the task.
Interactive game (software)
Rehabilitating engaging game which keeps a child motivated to perform exercises of pre-writing and writing.
The game evolves in several levels with increasing difficulty, depending on the progress and achievements of the patient.
Factors of interactivity:
- Sound, musical accompaniment and feedback during the exercises.
- Score points, earning badges, keys, collecting map pieces to accomplish the goals, discover the hidden treasures, gain awards etc.
- Celebration for successfully passed levels (visual, music, vibration), encouragement for attempts with a low score.
- Possibility to play in the network with friends (competitive factor).
Exercises types for basic skills recovery to implement into the game:

Pict. 4 A-F Types of exercises for the interactive game (Worksheets examples from "Rehabilitacion de la Disgrafia" by Portellano Perez, Quiros)
Trace the path, copy the trajectories, complete the symmetrical picture, connecting the dots as in example, unite the numbered points, find the way in the labyrinth; (Pict. 4 A,B,C)
Recognition of shape, size and colour: find and unite the figures of the same colour/shape/size. (Pict. 4 D)
Colouring pages (numbered colours on the picture in the related areas + specification card “number-colour”). (Pict. 4 E)
Rhythmic exercises (touching, giving taps: strong/weak, slow/fast; directly with finger or a pen aiming the points of a certain colour or size in the line sequence of points maintaining some simple rhythm. (Pict. 4 F)
Each patient has his personal virtual folder that contains therapeutic progress information; performance data such as accuracy, speed; calendar of activities, time of play. Each time logging into personal account, the previous results are shown and the game can be resumed exactly where it was left last time.
Possibility of remote monitoring of rehabilitation activities.
Development of use cases
Definition of the actors and their objectives (See pict. 5)
Actors interacting with system:
- Child-patient (Primary Actor)
- Doctor/therapist/parent (in role of administrator) in some use cases the child himself can perform the role of administrator.
Pict. 5 Diagram: Actors’ goals and steps to achieve them [click to enlarge]
Pict. 6 Use Case Diagram [click to enlarge]
Use cases scenarios (See diagram pict. 6)
Use case 1: Programming of robotic arm in Learning Mode (LM)
Actor: Administrator (Doctor/therapist/parent)
Goal: Teach robotic arm to perform specific writing or drawing movements, in order to create personalised exercises for individual therapeutic sessions.
Scenario:
- Admin: Logging into administrator’s account from the laptop which controls the robotic arm (insert user name and password).
- Admin: Launches the Learning Mode.
- Admin: Grasps the pen.
- Admin: Performs the desired movement.
- Admin: Controls the result (if satisfactory, proceeds with the next step, otherwise turns a step back).
- Admin: Saves the movement and introduces it in the context of custom exercise.
- Admin: Loads the custom level into the virtual folder of related patient.
Use case 2: Game activity (preliminary test, main game, personalised exercises)
Actor: Administrator (Doctor/therapist/parent); Child-Patient
Goal: Patient has to perform the game activity
Scenario:
- Admin (or patient if able to): Effectuates login into patient’s account (insert user name and password).
- Admin (or patient if able to): Launches preliminary test, or previously saved game, or personalised level.
- Patient: Grasps the pen.
- Patient: Performs the game activity in one of tree difficulty groups, passing from one to another when reaching the required conditions.
- Patient: Accomplishes the level – performance data is automatically saved into virtual personal folder; Next level unlocks for further playing.
- Patient: Finishes the game, all the performance data from the therapeutic session is being automatically saved into the patient’s virtual folder.
- Admin: Effectuates log out from patient’s account, closes the application on tablet, switches off the robotic arm and laptop (if necessary).
Robot-assisted exercises of handwriting
(Collaboration with engineers from NeuroLab of DIBRIS, University of Genoa)
Our partners, robotic engineers from Genoa NeuroLab were working simultaneously on a very similar project of writing assistance system, with the difference in application goals. They were focused on an inter-manual writing skill transfer (for people who for some reason have lost the capacity of writing with their dominant hand). See pict. 7 and video below.

Pict. 7 A Prototype of robotic system for assisted handwriting exercises.
Pict. 7 B Screenshots of cursive letters handwriting exercise
After confronting our prototype description (developed together with doctors and therapists from Infant Neuropsychiatry Department of Mondino National Neurological Institute of Pavia) with engineers from NeuroLab DIBRIS we were convinced that sharing our results may significantly improve their already existing hardware prototype and will lead to promising collaborative results.
The meeting was arranged in order to bring together all components of multidisciplinary team. Doctors and therapists from Mondino were expected to try and evaluate the prototype suggesting consequently ideas of improvement and proposing possible therapeutic protocol for the first try with dysgraphic children.
The meeting was held at Mondino Neurological Institute of Pavia. The portable prototype designed by NeuroLab DIBRIS was brought and installed in the office of prof. Ballotin (the Head of Infant Neuropsychiatric Department) to be presented and demonstrated in practice by engineers. While testing the prototype and discussing perspectives, several ideas for the joint research project emerged:
Pict. 8 Multidisciplinary meeting at Infant Neuropsychiatric Department of Mondino National Neurological Institute, Pavia.
- The device could be used not only for therapeutic exercises but also as a Diagnostic Tool for dysgraphia screening. For that purpose the prototype is already sufficient as it is, because the requirements for diagnostic tools are much less demanding than for rehabilitation once. The diagnostic test duration is relatively short (not more than 10 min) and only one single session is needed, so for this goal the factors of engagement, motivation, age appropriate interface design etc., became less significant.
- Doctors confirmed to have contacts with several local schools in Pavia area and the idea is to organize 2 or 3 days of diagnostic screening at one of these schools in order to individuate children with writing issues for the further participation in experimental project and to try the prototype for the first time on children, to see their reaction and the way they manage the device for eventual design corrections. Doctors suggested to prepare a test sessions 5-10 minutes long and apply them for screening of at least 50 children in 3rd to 5th grade of elementary school.
- Application of the robotic device for the rehabilitation treatment of writing disorders.
- The following rehabilitation protocol was preliminarily suggested: therapeutic sessions of 30 minutes each, 2-3 times a week for about 10 weeks with 8-12 children. In each session patient is supposed to exercises his pre-writing and/or writing skills (print letters and/or cursive) in different robotic assistive modes. In the beginning and in the end of treatment period patient’s writing skills and/or fine motor skills should be evaluated with specific tests in order to assess any improvements due to the therapy. It would be advantageous to involve also an age-matched control group.
- Changes in hardware of the system (Interventions of engineers and designer)
- Before the start of experiments it is expected to replace the current LCD monitor with a graphics tablet, in order to enable the recording of pen pressure and to increase the precision of movements control.
- Further changes are expected also in the pen grip in order to render it more handy and easy-managable (though this adjustment is not essential for the beginning of experiment).
- It was suggested to implement the possibility of external design personalization of robotic device, like e.g. animal-shaped cover, so younger children will appreciate it more, playing with funny and friendly personage (it was noted also that for boys the actual robotic exterior seems to be quiet attractive due to its futuristic, spaceship forms).
- Changes in user interface and game structure (Intervention of Designer, Engineers and Doctors)
- It was admitted that therapeutic exercises have to be age-appropriate, motivating and engaging, with the great variety of game activity. For the success of the treatment it is crucial to be able to get attention, interest and commitment of child in performing exercises. So the development of attractive game design is a must. For this purpose it was suggested to divide the exercises into levels with increasing difficulty. Each exercise will be a level of a video game, which can be passed only if the child has obtained a satisfactory result.
- Implementation of multi-player competitive mode in the network of friends is a great involving factor as well.
- One interesting feature of haptic device Falcon came out to be potentially useful for our project. The robotic system is capable of performing feedback simulations of different materials’ surfaces as well as simulation of different materials of endpoint grip (pen in our case), so we decided to take advantage of this option and add the possibility of exercising with different writing materials in order to enrich writing experience sensitively: e.g. writing with "wooden" pen on "water" surface or with "feather" pen on a "stone" surface.
- Age-appropriate graphics and game-storyline should be developed possibly with the involvement of end users (children in our case) and dedicated game designers.
To conclude the practical part of my thesis, I'd like to emphasize that Dysgraphia case study became a real substantive multidisciplinary project which keeps developing even after the accomplishment of present doctoral thesis. The results of prototype testing in school should be available for analysis soon, in the meanwhile the plans of hardware and software improvement are in an active phase of realization.
Conclusions, Recommendations
The answer to the essential question of this doctoral thesis “What is the role of designer in project development of rehabilitation programs (or any other project field)?” will be the following:
Designer plays the conductive role between different groups of specialists of various competences and frames of reference (e.g. engineers, software developers, doctors, therapists etc.), and communities of individuals with particular characteristics (potential users or customers: patients, children, parents etc.), uniting them together as a productive multidisciplinary team and contributing knowledge of his own competence (product design, graphic design, interface design, user experience design, ergonomics etc.) (See the diagram Pict. 9)
In order to be able to organize, manage and be a valuable part of the project team, designer should inevitably become a multidisciplinary researcher as well.
Answering the main research questions:
How design can contribute to children’s neurological rehabilitation?
Present research exposed the example of successfully developing multidisciplinary project of robotic rehabilitation system for Dysgraphia. In our case the therapeutic equipment for certain neurological disorder in a certain infant neuropsychiatric department is being brought to a new quality level. Consequently patient’s therapeutic experience is to become more pleasant and exciting, so the efficiency of rehabilitation process is being improved.
Moreover our suggestion is that use of our general guidelines of project development would bring to similar positive results in other fields of industry/activity.
Summarizing the results and analyzing the research framework afterwords we came to the conclusion that in can be categorized as Action Research.

Pict. 10 Action Research model
Action Research - is either research initiated to solve an immediate problem or a reflective process of progressive problem solving led by individuals working with others in teams or as part of a “community of practice” to improve the way they address issues and solve problems. Action research strategy's purpose is to solve a particular problem and to produce guide-lines for best practice.
The essentials of action research design follow a characteristic cycle whereby initially an exploratory stance is adopted, where an understanding of a problem is developed and plans are made for some form of interventionary strategy. Then the intervention is carried out (the "action" in Action Research) during which time, pertinent observations are collected in various forms. The new interventional strategies are carried out, and this cyclic process repeats, continuing until a sufficient understanding of (or a valid implementation solution for) the problem is achieved. The protocol is iterative or cyclical in nature and is intended to foster deeper understanding of a given situation, starting with conceptualizing and particularizing the problem and moving through several interventions and evaluations. (See pict. 10)
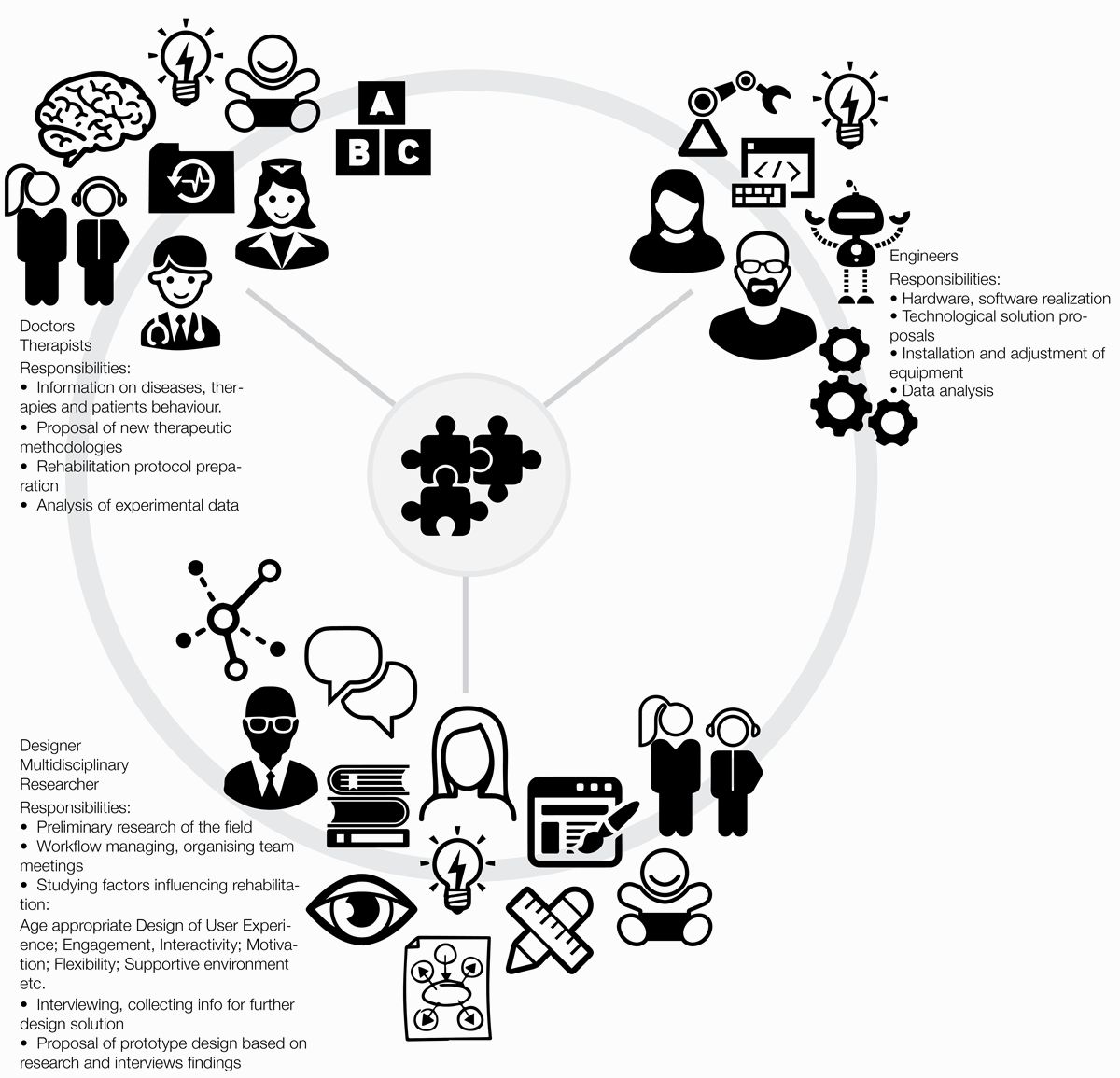
Pict. 9 Schematic diagram of project development team participants and their responsibilities. Co-designing robotic rehabilitation program for children with dysgraphia.
RECOMMENDATIONS
Research Design. Generalizing guide-lines.
Pict. 11 [click to enlarge] Diagram: Generalized steps of accomplished action research (from the bottom -> to the top)
The research design refers to the overall strategy that you choose to integrate the different components of the study in a coherent and logical way, thereby, ensuring you will effectively address the research problem; it constitutes the blueprint for the collection, measurement, and analysis of data. Research problem determines the type of design (Action Research Design, Case Study Design, Causal Study Design, Cohort Design, Cross-Sectional Design, Descriptive Design, Experimental Design, Exploratory Design, Historical Design, Longitudinal Design, Observational Design, Philosophical Design, Sequential Design). Research design is the framework that has been created to seek answers to research questions.
Research Design of my accomplished study is recognized as an Action Research with the following generalized research questions:
How design can contribute to the field of issue?
Generalized conducting questions:
- What are the factors influencing the object of issue in the respective field?
- What are the main benefits and drawbacks of existing solutions?
- How the drawbacks can be eliminated or reduced?
- How the benefits can be forced?
- Which technologies can be applied for the eventual improvement of object at issue?
- Which design methodological approaches can be applied in order to improve the project development process?
- What is the role of designer in the project development?
The diagram (Pict. 11) shows four main generalized steps of my study.
The most important applied research methods were: Literature review, Analysis, Field research, Observation and Participatory observation, Participatory action research, Interview, Creative participation, co-design.
The proposed research model is obviously very general, flexible and incomplete, number of steps and participants on every step may vary, for example it is always advantageous to consider end user’s opinion right from the very first step and through the whole project’s lifecycle.